Medical equipment that obtains highly reliable objective measurements indicating if the retina, optic nerve, or visual pathway is healthy or damaged.
Electrophysiologic testing enables early and more accurate diagnosis especially for difficult cases.
In contrast to subjectively reported or measured visual functions (such as acuity, contrast sensitivity, color vision, or field of vision), for decades modern medicine has used objective evaluation of the functionality of the visual system through electrophysiological examination (EE).
Such instrumentation performs diagnostic tests for the entire visual system starting from examining different retinal cells (electroretinogram - ERG), measuring conductivity along the optic nerve (flash visual evoked potentials - fVEP) and assessing the primary visual cortex (pattern VEPs).
The major benefit of objective visual assessment is that visual function may be determined without relying on subjective responses from the patient.
Major Benefits of Electrophysiologic Testing:
1
Highly reliable objective results
Obtained results are reliable and objective to test if the retina or optic nerve is healthy or damaged
2
Early diagnosis of eye conditions
Early diagnosis of different types of optic neuropathies or inherited retinal conditions
3
Gold standard for kids
Especially beneficial when testing infants and kids who are unable to verbalize visual complaints
4
Diagnosis and monitoring
Electrophysiological diagnostic testing aids in unexplained vision loss or in unclear cases
5
Beneficial if lens is not clear
Its indispensable if a patient’s lens or vitreous is not transparent enough to perform funduscopic evaluation
6
Testing is much less stressfull
Because it does not require subjective feedback patients are confident and relaxed
When electrophysiologic testing is required
To differentiate retinal and optic nerve disorders
To determine the cause of unexplained vision loss or if test results are unreliable
To evaluate the visual system in infants with questionable vision or young children
To assess the visual system with uncooperative patients
To determine the cause of vision loss when opaque media prevents other testing
In cases of marginal or borderline results from normal ophthalmological tests
When suspecting early-stage retinal dystrophy despite normal routine testing
In unilateral vision loss from suspected multiple sclerosis (first diagnosis or relapse)
In cases of sub-clinical or preclinical eye conditions (glaucoma, AMD, etc)
To assess retinal function and improve management in severe diabetic retinopathy
When vision complaints are inconsistent with visible structural abnormalities
When suspecting an intracranial lesion, traumatic brain injury, or toxic damage
When testing is recommended
If risk for developing eye conditions such as inherited retinal dystrophies is high
For patients with vascular diseases or transient vision loss
To confirm amblyopia in adolescents or adults
In cases of chronic retrobulbar optic neuritis
To differentiate ocular conditions from systemic or traumatic conditions
For patients experiencing visual disturbances but with absent or minor ocular findings
To obtain a more specific diagnosis for optic nerve or visual pathway disorders
When you can spare on testing
If vision problems are consistent with an established and confirmed diagnosis
If your routine eye examinations reveal no ocular or visual abnormalities
If the current diagnosis and management are sufficient and successful
If child patients are cooperative and results are reliable
In cases of stabile structural retinal or optic nerve abnormalities
If vision has been stable and unconcerning over many years
Electrophysiologic testing is very effective at identifying patients for early intervention because it can detect retinal or optic nerve changes many months (or even few years) prior to ophthalmic complaints and even structural abnormalities.
Frequently Asked Questions about electrophysiological examination
What is an electroretinography (ERG) test?
An ERG is a painless, safe, and non-invasive form of electrophysiological testing conducted to assess the function of the retina. The retina is a transparent structure in the back of the eye responsible for converting light into electrical signals. An ERG is similar to an EKG or EEG, but for the retina. There are several types of ERGs including full field (flash), pattern, multifocal, photic-negative response, amongst others. With an ERG, light stimulates the retina and the electrical responses are measured.
What is a Visual Evoked Potentials (VEP) test?
Another electrophysiological test is the visual evoked potential (VEP) which is similar to the ERG, but measures the electrical signal of the optic nerve and brain, rather than the retina. After an electrical signal is formed in the retina, this signal travels to the primary visual cortex of the brain via the optic nerve. Therefore, the VEP is a diagnostic test assessing the signaling from the optic nerve to the primary visual cortex of the brain. This form of electrophysiological evaluation is especially useful when vision loss is suspected to be due to an optic nerve or brain condition. Similar to the ERG, this is a non-invasive, safe, and painless procedure with no side effects.
Will this replace any other eye tests I take?
Electrophysiological testing is performed in addition to other diagnostic tests such as perimetry (visual field) and OCT testing. ERG and VEP further assess your eye health through evaluation of your retina and optic nerve function. These tests are especially useful for accurate diagnosis and management of specific eye conditions. Electrophysiological testing is also extremely helpful in early disease states or when the cause of vision loss is unknown. Electrophysiological testing assesses the function, rather than the structure, of the retinal layers, optic nerve, and visual pathway to the brain. This information is used to determine which part of the visual pathway is responsible for vision loss and to what degree vision may be affected.
How should I prepare for the test?
Unless otherwise directed by your physician, continue taking all medications. Avoid hair products and make sure your hair is clean and without ponytails or braids. Dress comfortably. Young children can have calming items such as a blanket, toy, or pacifier. Small children will be allowed to sit in the lap of a parent during testing. lease Please bring your current glasses if possible. This is helpful for the technicians. Depending on the initial testing results, the technician may have you wear a trial frame with lenses during the remainder of the exam.
How many tests will I have and how long does it take?
The number and types of diagnostic tests needed is dependent on your diagnosed or suspected condition(s). Multiple tests may be performed during your appointment or at separate visits. Therefore exam time varies patient to patient. It is generally best to assume an appointment time of at least an hour.
How is a full-field ERG done?
Full field ERGs are performed with patients comfortable lying down or sitting up. The eyes may be dilated and the patient may sit in a dark room for 20 minutes to “dark-adapt”. The eyes may be numbed with drops. Several electrodes (either contact lenses or wires) are gently placed on the eyes and one electrode is placed on the forehead. Although the test is painless, sometimes patients have a sensation similar to an eyelash being in the eye from the electrodes. Testing is typically done one eye at a time. The patient will then look at a target and see flashes of light designed to stimulate the retina. The flashes start very dim and slowly become brighter. The retinal responses received by the electrodes are interpreted and displayed on a computer screen. This part takes 10-15 minutes. The test may be repeated after the patient is “light-adapted” and with the lights on. During this time flickering lights may also be used. This again takes 10-15 minutes. Rod photoreceptors are tested in the dark with dim light while cone photoreceptors are tested in a normally lit room with brighter lights or flickering lights. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing.
How is the mfERG done?
Similar to full field ERGs, patients are seated comfortably and electrodes are placed on the eyes and forehead. Testing is performed one eye at a time. The patient will look at a target on the screen (usually an ‘X’) and the screen will display a flashing hexagon pattern for 30 seconds. This test is usually repeated 8 times per eye. The total testing time is approximately one hour. Data is displayed using waveform traces or colored graphs. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing.
What else do I need to know?
The most important thing is to relax. This helps ensure reliable test results and an efficient exam. Please refrain from applying makeup or hair products. Please do not rub your eyes after the testing. Our supplies are latex-free, hypo-allergenic, and water soluble. Please inform our staff of any allergies you may have.
Electrophysiological testing is contraindicated in patients with a history of seizures. Electrophysiological testing is safe for pregnant women and persons with a pacemaker, but please consult with your primary care physician prior to testing.
Please notify us of any recent changes in vision or eye concerns prior to testing. Eye dryness, itchiness, allergies, or irritation may affect results and may need to be treated prior to testing.
Are these vision tests covered by my insurance?
Although each medical insurance plan is different, many insurances cover electrophysiological tests especially when such testing is warranted to determine appropriate diagnosis, treatment, or management. Our office can help verify coverage by your insurance.
Not sure if you need electrophysiologic testing?
When testing is helping differentiate diseases of retina or optic nerve in children
VEP and ERG testing is exceptionally advantageous with certain young, cognitively impaired, nonverbal, and elderly patients. Reliance on patient history and subjective responses proves time consuming and unreliable in some circumstances. Electrophysiological Examination improves accurate diagnosis, management, clinical efficiency, and overall patient care in cases of unreliable subjective responses (needed for visual acuity and perimetry). Additionally, electrophysiological testing has proven beneficial in patients with complicated optic nerve, retinal, or ...
visual cortex conditions not easily understood or observed through traditional clinical evaluation or ocular imaging. Conditions can also be monitored with EE to assess progression, resolution, or stabilization. Restore Vision Clinic has the capability using electrophysiology to also monitor response to therapy to ensure functional visual improvement for patients.
Diagnosis through Electrophysiology
Whereas most ocular imaging involves capturing a photo or scan to assess the structure or clinical appearance of ocular tissue, EE actually assesses the function of ocular (retina) and brain (pathways) tissue. Oftentimes initial structural changes of the visual system remain undetectable though routine assessment of visual functions. This is especially true in early disease processes, such as pre-perimetric glaucoma or some forms of macular dystrophy. Electrophysiology is especially useful in the early diagnosis of conditions before abnormalities are observable with clinical examination or OCT.
Similarly, another valuable parameter at an early disease stage demonstrable by VEP and ERG testing is unexplained asymmetry between the eyes, an indicator of an early abnormality. This data is advantageous in not only diagnosing uncommon ocular and neurological disorders, but also earlier diagnosis of such conditions. Sometimes visual field loss presents with difficulty attributing such loss to either retina or optic nerve damage due to indistinguishable or minor structural abnormalities. In these cases, comprehensive electrophysiological examination (EE) differentiates sources of vision deterioration, thus improving proper therapy and management. Last but not least, electrophysiology is exceptionally helpful in ruling out suspected ocular and neurological conditions when other assessments proved unsuccessful.
Traveling From The Eye To The Brain
Eye and retina
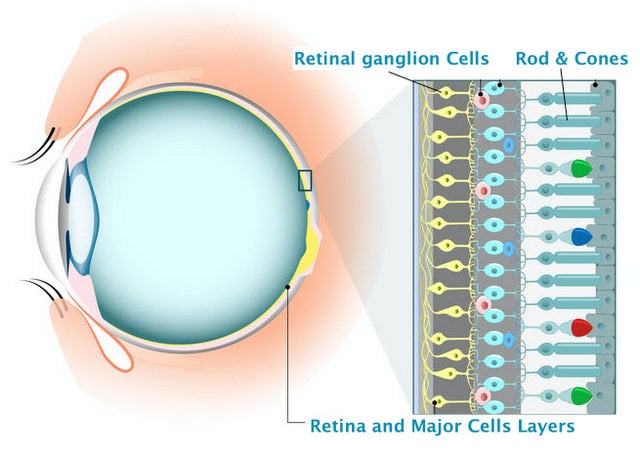
Electroretinograms (ERG) are based on nearly direct (through sclera) recordings of retinal cellular activity in response to flashes of differing intensities or white-black patterns. ERGs test retinal cells throughout the retina – macula, perimacula, and the entire retina. In addition to assessing certain areas of the retina, ERGs also evaluate specific retinal cells and layers. Specific waves of ERG are known to correspond with specific retinal cells such as rods, cones, Muller, bipolar, RPE, amacrine, and ganglion. Information from specific retinal layers aids clinicians in discerning which specific maculopathy, inherited retinal disease, or retinal degeneration may be occurring.
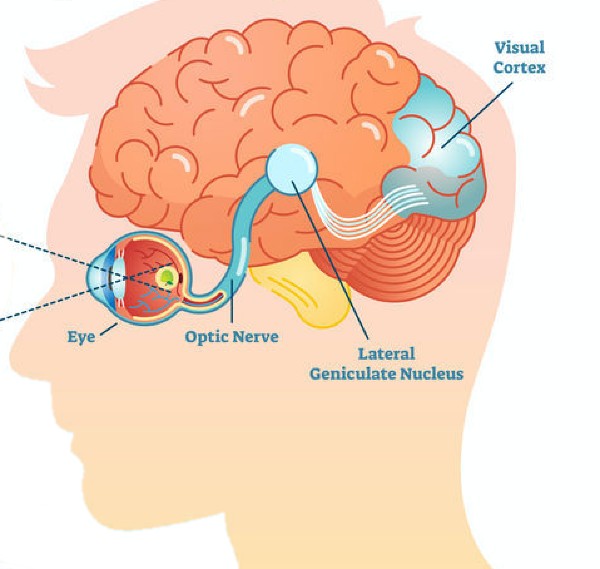
The key difference between visual evoked potentials (VEP) from ERG is that VEPs are recorded from the back of the head, where the primary visual center, known as occipital lobe, is located. Signals originating at the retina must travel through the whole visual pathway – the optic nerve, cross at the optic chiasm, the optic tract, and finally through the subcortical brain pathway to reach the occipital lobe. Results of VEPs have diagnostic and management applications for inflammatory optic neuropathies (i.e. optic neuritis), infantile optic nerve hypoplasia, cortical visual impairment, amblyopia, and cerebral strokes. Although, any medical condition associated with damage behind the eye (optic nerve and visual pathway disorders) can be assessed and monitored with VEP.
Optic nerve and brain
Visual Evoked Potentials
Flash Visual Evoked Potentials
This test measures the conductivity along the optic nerve. Latency and amplitude are used for assessment. Latency describes the length of time it takes for a signal to travel from the retina to the visual cortex. Amplitude describes the magnitude of signal response to the stimulus. Certain pathological conditions result in diminished latency while other conditions cause diminished amplitude or both.
Pattern Visual Evoked Potentials
This test assesses the primary visual cortex (occipital lobe) in regard to quality of visual acuity. It also measures functionality of the central part of the optic nerve
Electroretinogram
Depending on clinical needs there are four major ERG examinations: a) Full Field ERG, b) Photopic Negative Response (PhNR), c) Pattern ERG, and d) Multifocal ERG.
Full Field ERG
Full Field ERG is aimed to test photoreceptors. The report reveals an initial negative wave, called the a-wave, which is produced by the cone and rods. An abnormality of photoreceptors (caused by different types of retinal dystrophies) affects the a-wave response. Full Field ERG is a sufficient tool in establishing a diagnosis of retinal pathology.
Photopic Negative Response (PhNR)
PhNR shows generalized activity of retinal ganglion cells and their axons, which are exceptionally vulnerable in early stages of disease with glaucoma, hereditary optic neuropathies (ex. Leber Optic Atrophy), and other types of optic neuropathies.
Multifocal ERG
A special type of ERG is the multifocal ERG which utilizes flickering hexagons of various sizes to elicit responses from multiple, focal retinal locations. Obtaining focal responses defines the involved and damaged areas of the retina, determining if such damage is local or diffuse.
Pattern ERG (pERG)
The pattern ERG elicits responses from cones, bipolar cells, and – more importantly – retinal ganglion cells. Because it only measures responses of the central retina, it is useful in determining macular dysfunction. Moreover, sensitivity of pERG to detect and measure ganglion cell function is crucial for glaucoma and optic nerve disease.
What Physicians Are Saying
“I have known Dr. Dr. Anton Fedorov for many years and his reputation as a specialist in field of vision restoration. He is pioneer in the area of non invasive electrical stimulation therapy. For more than 20 years, he has successfully used Restoration Therapy to help patients regain vision-loss from ‘untreatable’ conditions. We provide long lasting collaboration with him in regard to execute follow up evaluation for our mutual patients and help him exam his potential here in London if they can be qualified to receive treatment in Berlin Germany."
.jpeg)
 Full field ERGs are performed with patients comfortable lying down or sitting up. The eyes may be dilated and the patient may sit in a dark room for 20 minutes to “dark-adapt”. The eyes may be numbed with drops. Several electrodes (either contact lenses or wires) are gently placed on the eyes and one electrode is placed on the forehead. Although the test is painless, sometimes patients have a sensation similar to an eyelash being in the eye from the electrodes. Testing is typically done one eye at a time. The patient will then look at a target and see flashes of light designed to stimulate the retina. The flashes start very dim and slowly become brighter. The retinal responses received by the electrodes are interpreted and displayed on a computer screen. This part takes 10-15 minutes. The test may be repeated after the patient is “light-adapted” and with the lights on. During this time flickering lights may also be used. This again takes 10-15 minutes. Rod photoreceptors are tested in the dark with dim light while cone photoreceptors are tested in a normally lit room with brighter lights or flickering lights. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing.
Full field ERGs are performed with patients comfortable lying down or sitting up. The eyes may be dilated and the patient may sit in a dark room for 20 minutes to “dark-adapt”. The eyes may be numbed with drops. Several electrodes (either contact lenses or wires) are gently placed on the eyes and one electrode is placed on the forehead. Although the test is painless, sometimes patients have a sensation similar to an eyelash being in the eye from the electrodes. Testing is typically done one eye at a time. The patient will then look at a target and see flashes of light designed to stimulate the retina. The flashes start very dim and slowly become brighter. The retinal responses received by the electrodes are interpreted and displayed on a computer screen. This part takes 10-15 minutes. The test may be repeated after the patient is “light-adapted” and with the lights on. During this time flickering lights may also be used. This again takes 10-15 minutes. Rod photoreceptors are tested in the dark with dim light while cone photoreceptors are tested in a normally lit room with brighter lights or flickering lights. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing. Similar to full field ERGs, patients are seated comfortably and electrodes are placed on the eyes and forehead. Testing is performed one eye at a time. The patient will look at a target on the screen (usually an ‘X’) and the screen will display a flashing hexagon pattern for 30 seconds. This test is usually repeated 8 times per eye. The total testing time is approximately one hour. Data is displayed using waveform traces or colored graphs. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing.
Similar to full field ERGs, patients are seated comfortably and electrodes are placed on the eyes and forehead. Testing is performed one eye at a time. The patient will look at a target on the screen (usually an ‘X’) and the screen will display a flashing hexagon pattern for 30 seconds. This test is usually repeated 8 times per eye. The total testing time is approximately one hour. Data is displayed using waveform traces or colored graphs. The results are then analyzed and interpreted by your eye care professional. Patients do not need to do anything to prepare for ERG testing except not wear makeup before the testing and not rub their eyes after the testing.