NAION classically presents immediately upon wakening as moderate vision loss in one eye and generally progresses for several hours to days, and possibly even weeks. The degree of initial central vision loss and level of central visual recovery varies widely. The IONDT study found that initial NAION visual acuities ranged from 20/20 to light perception only with approximately 50% of patients having a visual acuity of 20/64 or better and two-thirds of patients having a visual acuity of 20/200 or better. Another study found that two weeks after initial symptom onset, almost 50% of NAION patients have a visual acuity of 20/30 or better. For this reason, consideration of alternative optic neuropathies is warranted in cases of prolonged and severe central vision loss.
 Patients generally present with a painless and sudden onset of vision loss in one eye accompanied by peripheral vision disturbances, noticed in the morning by over 66% of patients. Although eye pain is rare in NAION, approximately 8-12% of patients report periocular eye pain which may initially make AION difficult to discern from optic neuritis. However in NAION, unlike optic neuritis, patients never present with pain during eye movements.
Patients generally present with a painless and sudden onset of vision loss in one eye accompanied by peripheral vision disturbances, noticed in the morning by over 66% of patients. Although eye pain is rare in NAION, approximately 8-12% of patients report periocular eye pain which may initially make AION difficult to discern from optic neuritis. However in NAION, unlike optic neuritis, patients never present with pain during eye movements.
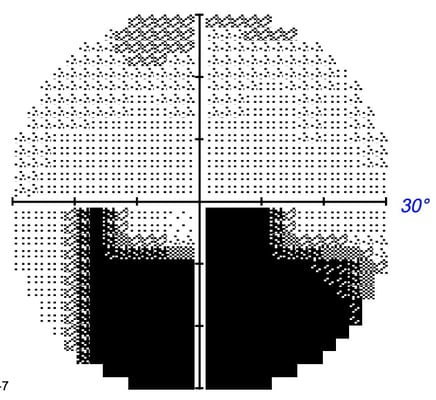
In addition to central and peripheral vision changes, patients also commonly display color vision loss in the form of mild to moderate dyschromatopsia which is generally correlated with the level of visual acuity loss. A relative afferent pupillary defect is generally observed in the affected eye. Any form of optic nerve associated visual field loss may also occur in AION, but field defects commonly respect the horizontal midline and present as nerve bundle fiber defects, similar to glaucomatous visual field defects. The most frequently observed types of visual field abnormalities associated with NAION are inferior altitudinal or inferior arcuate defects.
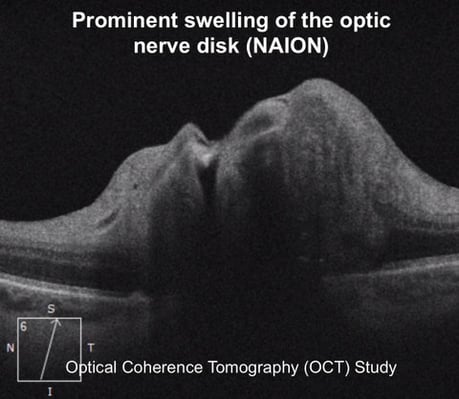
As revealed in the name, the most anterior portion of the optic nerve, known as the “optic disc” is the site of involvement in AION. 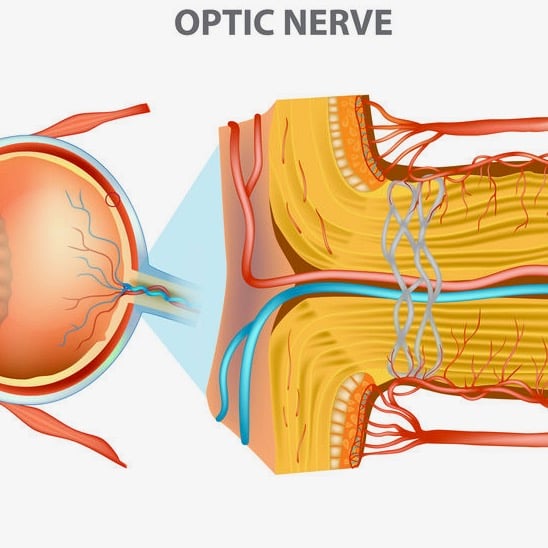 This is evident during examination of the fundus as optic disc edema, oftentimes with optic disc hyperemia and peripapillary splinter-shaped hemorrhages. This disc edema usually resolves in 4-6 weeks with sectoral or diffuse optic disc pallor potentially being sequelae. Although uncommon, cotton wool spots (evidence of retinal ischemia) may also be present. AION incidents are far more common in persons with a physiologically small cup-to-disc ratio, the area of the optic nerve where axons enter the eye. While a normal ratio is approximately 0.3, a ratio less than 0.25 is considered a “crowded disc” or a “disc at risk” for an AION episode. Recurrence of AION episodes in the affected eye are rare, estimated to be only 3-8%. However, the likelihood of involvement of the fellow eye over the following 5 years ranges from 15-24%.
This is evident during examination of the fundus as optic disc edema, oftentimes with optic disc hyperemia and peripapillary splinter-shaped hemorrhages. This disc edema usually resolves in 4-6 weeks with sectoral or diffuse optic disc pallor potentially being sequelae. Although uncommon, cotton wool spots (evidence of retinal ischemia) may also be present. AION incidents are far more common in persons with a physiologically small cup-to-disc ratio, the area of the optic nerve where axons enter the eye. While a normal ratio is approximately 0.3, a ratio less than 0.25 is considered a “crowded disc” or a “disc at risk” for an AION episode. Recurrence of AION episodes in the affected eye are rare, estimated to be only 3-8%. However, the likelihood of involvement of the fellow eye over the following 5 years ranges from 15-24%.
An interesting and distinct entity similar to NAION exists known as incipient NAION where despite a crowded optic nerve being edematous, visual function remains unaffected. In these cases of asymptomatic optic disc edema occurring in a “disc at risk”, half of the time the disc swelling quickly resolves with no recurrence. A quarter of the time the disc swelling resolves but recurs later with symptoms. The final quarter of the time the initial disc swelling ends up progressing to symptomatic NAION. For reasons that are not well understood, incipient NAION is more likely to occur in diabetic patients and younger patients are more likely to progress to NAION than older patients.
Due to the heightened risk of the fellow eye being affected, patients being evaluated for NAION should promptly undergo complete blood count, erythrocyte sedimentation rate, and C-reactive protein diagnostic testing to rule out AAION or “giant cell arteritis”.
The risk of spontaneous NAION is increased by conditions, events, or medications which may reduce perfusion to the anterior optic nerve through microvascular blood-flow disruption. These risk factors include:
There does not appear to be any gender predilection as NAION occurs fairly equally amongst men and women. Although AION may occur at any age, the average age of onset is between 57-67 years despite the fact that one study found that 23% of AION patients are under the age of 50. Caucasions also appear to have an increased risk, likely due to optic disc anatomy.
AION is a vascular optic neuropathy -- therefore systemic vasculopathic conditions predispose a person to AION. According to IONDT, 60% of NAION patients had at least one vasculopathic risk factor. Among the vasculopathies associated with ischemic small vessel conditions, the most notable include diabetes, hypertension, and hypercholesterolemia.  47-49% of NAION patients have hypertension while 24-26% have diabetes. Other potential, but unconfirmed risk factors include arteriosclerosis, lipohyalinosis, smoking, vascular autoregulation failures, sleep apnea, vasospasm, anemia, nocturnal hypotension, and generalized hypoperfusion.
47-49% of NAION patients have hypertension while 24-26% have diabetes. Other potential, but unconfirmed risk factors include arteriosclerosis, lipohyalinosis, smoking, vascular autoregulation failures, sleep apnea, vasospasm, anemia, nocturnal hypotension, and generalized hypoperfusion.
Research indicates that nocturnal systemic hypotension likely plays a major role in NAION development, especially in people with dramatic nocturnal dips. Normally occurring hypotension may disrupt blood circulation and perfusion pressure to the anterior optic nerve (i.e. the optic disc).  Patients previously diagnosed with optic nerve circulation disorders or systemic hypotension have a heightened risk of NAION development. One major cause for concern is nocturnal hypotension secondary to antihypertensive medicinal therapy -- medications frequently used by individuals in age range for NAION development. Aggressive antihypertensive treatment or medications administered in the evenings may provoke an NAION episode by exagerrating normal systemic nocturnal hypotension. In hypertensive patients with NAION, studies indicate that those patients with visual field loss demonstrate significantly lower blood pressure than those patients with no visual field loss. This research suggests that certain individuals may be at increased risk of both NAION development and NAION progression due to exaggerated nocturnal hypotension, especially in cases of aggressive hypertension treatment.
Patients previously diagnosed with optic nerve circulation disorders or systemic hypotension have a heightened risk of NAION development. One major cause for concern is nocturnal hypotension secondary to antihypertensive medicinal therapy -- medications frequently used by individuals in age range for NAION development. Aggressive antihypertensive treatment or medications administered in the evenings may provoke an NAION episode by exagerrating normal systemic nocturnal hypotension. In hypertensive patients with NAION, studies indicate that those patients with visual field loss demonstrate significantly lower blood pressure than those patients with no visual field loss. This research suggests that certain individuals may be at increased risk of both NAION development and NAION progression due to exaggerated nocturnal hypotension, especially in cases of aggressive hypertension treatment.
The exact underlying mechanism(s) responsible for ischemia in AION is undetermined.
Proposed ischemic mechanisms include:
- embolization
- vasospasm
- autoregulation dysfunction
- localized arteriosclerosis
- general hypoperfusion
- venous circulation occlusion or
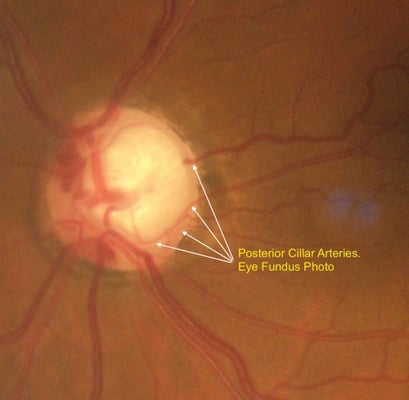
any combination of these mechanisms resulting in a circulatory insufficiency or infarct within the retrolaminar region of the optic nerve head which is supplied by the short posterior ciliary arteries.  Although the precise mechanism is unclear, “discs at risk” or crowded optic discs are more susceptible to ischemia possibly due to mechanical stress of the local circulatory system. Sleep apnea commonly causes recurrent nocturnal ischemic episodes and may be associated with NAION.
Although the precise mechanism is unclear, “discs at risk” or crowded optic discs are more susceptible to ischemia possibly due to mechanical stress of the local circulatory system. Sleep apnea commonly causes recurrent nocturnal ischemic episodes and may be associated with NAION.
Unremitting hypoperfusion to the optic disc is dependent on dysfunction of the normal optic nerve head autoregulatory function; known to be impaired by antihypertensive medications, vasospasms, and arteriosclerosis. This local autoregulatory system typically maintains steady blood flow despite fluctuating perfusion pressures, metabolic conditions, and intraocular pressure. Disruption of this autoregulatory system may result in persistent hypoperfusion of the optic disc.
NAION related optic nerve damage occurs in two ways. Firstly, initial optic nerve ischemia and subsequent hypoxia causes axonal injury evidenced by optic nerve edema. 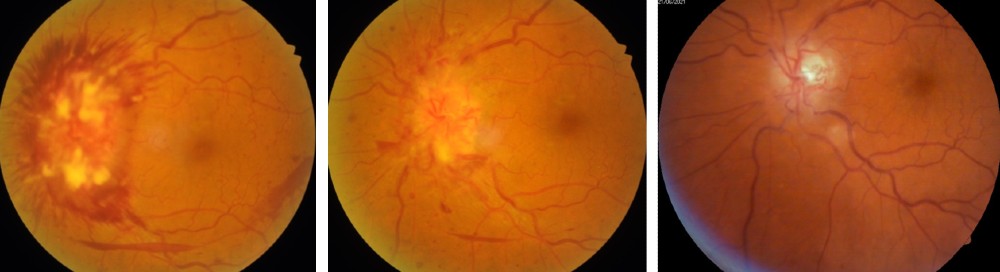 Secondly, this edema impairs the transportation of essential nutrients and neurotransmitters to retinal ganglion cells thus damaging the retinal ganglion cell layer by means of oxidative stress, excitotoxicity, metabolic imbalances, mitochondrial failure, or apoptosis.
Secondly, this edema impairs the transportation of essential nutrients and neurotransmitters to retinal ganglion cells thus damaging the retinal ganglion cell layer by means of oxidative stress, excitotoxicity, metabolic imbalances, mitochondrial failure, or apoptosis.
A small cup-to-disc ratio exists in most patients who proceed to develop NAION. Some studies suggest the mechanism to be compartment syndrome - a condition in which the pressure within a given space increases resulting in mechanical damage or blood flow disruption. Within the orbit, compartment syndrome may lead to cyclical swelling and ischemia with possible subsequent infarction. Histopathologic examination has revealed cavernous degeneration and axonal compression in the laminar region of the optic nerve in patients with NAION.
Although small cup-to-disc ratios and optic disc crowding is the primary risk factor for NAION development, other ocular risk factors exist such as disc edema, posterior vitreous detachments, and optic disc drusen. NAION episodes are also associated with certain ocular procedures including cataract extraction, laser-assisted in situ keratomileusis (LASIK), intravitreal injections, and strabismus surgery.
 The ophthalmic artery branch of the internal carotid artery is responsible for the vast majority of the blood supply to the optic nerve. The inner retinal layers receive blood flow from a branch of the ophthalmic artery called the central retinal artery, which enters the optic nerve roughly one centimeter behind the globe. However, the outer retinal layers depend on the choroidal arteries, which stem from the posterior ciliary arteries, for blood supply.
The ophthalmic artery branch of the internal carotid artery is responsible for the vast majority of the blood supply to the optic nerve. The inner retinal layers receive blood flow from a branch of the ophthalmic artery called the central retinal artery, which enters the optic nerve roughly one centimeter behind the globe. However, the outer retinal layers depend on the choroidal arteries, which stem from the posterior ciliary arteries, for blood supply.
From the ophthalmic artery to the choroid, branches of the posterior ciliary artery run along and penetrate the optic nerve. The pial plexus supplies the posterior portion of the optic nerve through small branches off the ophthalmic and posterior ciliary arteries. However, the centermost area of the posterior optic nerve is more susceptible to ischemia than the anterior optic nerve due to a limited number of capillaries penetrating and eventually extending to the innermost tissue in this area.
The blood supply of the most anterior portion of the optic nerve, the optic disc or optic nerve head, derives from the Circle of Zinn-Haller, an arterial circle formed by anastomoses of short posterior ciliary artery branches, pial arterial network branches, and choroidal vessel branches. Local vasculopathies such as atherosclerosis and vasculitis are known to affect these tiny arteries which are too small for emboli to reach.
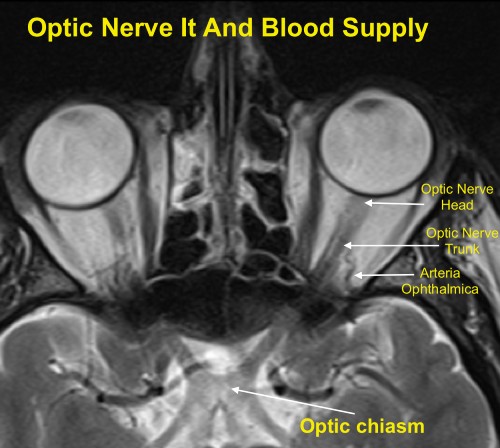 Ischemic optic neuropathy (ION) may present during hypoperfusion of the ophthalmic artery or its subsequent branches. The clinical signs and patient symptoms vary depending on the region of the optic nerve in which the ischemia occurs. The optic disc appears normal in cases of posterior optic nerve ischemia while the optic disc is edematous in cases of anterior optic nerve ischemia.
Ischemic optic neuropathy (ION) may present during hypoperfusion of the ophthalmic artery or its subsequent branches. The clinical signs and patient symptoms vary depending on the region of the optic nerve in which the ischemia occurs. The optic disc appears normal in cases of posterior optic nerve ischemia while the optic disc is edematous in cases of anterior optic nerve ischemia.
In some rare instances, such as NAION development in acute angle closure glaucoma, increased intraocular pressure may reduce blood supply to the optic disc. The cup-to-disc ratio, where a small ratio predisposes a patient to NAION, is dependent on the size of the optic disc and the scleral canal. This is a physical ratio of the diameter of the central cup to the overall optic disc observed during fundoscopy. Within the scleral canal resides the meshlike lamina cribrosa tissue which supports the optic nerve. The total volume of the optic nerve tissue is relatively constant between normal eyes. Thus, a small scleral canal yields a small cup-to-disc ratio while a large scleral canal yields a large cup-to-disc ratio. Small cup-to-disc ratios, more common in white individuals than black individuals, significantly increase the risk of NAION development which likely explains why white individuals are more likely to suffer from NAION.
 The optic disc swelling accompanying NAION may be diffuse or segmental with or without hyperemia. Pallor may occur after resolution of the disc edema or, rarely, during the disc edema. Peripapillary splinter hemorrhages are commonly observed while cotton wool spots and macular hard exudates are seldom found. In more advanced cases, retinal arterioles may be narrowed. The contralateral eye (i.e. the non-affected eye) usually reveals a small cup-to-disc ratio or a “disc at risk.”
The optic disc swelling accompanying NAION may be diffuse or segmental with or without hyperemia. Pallor may occur after resolution of the disc edema or, rarely, during the disc edema. Peripapillary splinter hemorrhages are commonly observed while cotton wool spots and macular hard exudates are seldom found. In more advanced cases, retinal arterioles may be narrowed. The contralateral eye (i.e. the non-affected eye) usually reveals a small cup-to-disc ratio or a “disc at risk.”
The “disc at risk” or “crowded disc” is thought to make the optic nerve head susceptible to ischemia from structural crowding of the axons in the lamina cribrosa layer. While in the majority of cases visual symptoms presumably occur during the onset of optic nerve head edema, incipient NAION, as mentioned previously, is defined as an edematous “disc at risk” in the absence of visual symptoms. Approximately half of patients with incipient NAION never develop visual symptoms and have complete resolution of their disc edema. Conversely, the other roughly half of incipient NAION cases may be considered to be in a presymptomatic phase of NAION as visual symptoms eventually arise with either this episode of disc edema or during a future ischemic event.
When considering NAION as a diagnosis, a meticulous medical and social history is needed in addition to a thorough eye examination. Questioning pertaining to sleep apnea, giant cell arteritis (GCA), and erectile dysfunction drugs is warranted.
 Although NAION may present with findings similar to that of GCA, a classic presentation of NAION without GCA signs or symptoms may not warrant the usual GCA testing of a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). However, if there is any doubt then CBC, ESR, and CRP testing is indicated to rule out GCA. Patients should always be evaluated by a primary-care physician for potential modifiable or treatable risk factors including smoking, sleep apnea, hypertension, diabetes, hyperlipidemia, and other vascular disorders. Neuroimaging is only performed in cases diverging from a typical NAION course such as prolonged optic disc edema, progressing vision loss, or unusual pain. Except in cases of family history or personal clinical evidence, there is no proven value of additional vasculopathic or prothrombotic diagnostic testing (ex. carotid studies, hypercoagulability testing), however homocysteine levels may be tested in patients under the age of 50. Patients with significant hyperhomocysteinemia may be recommended supplementation of vitamins B6, B12, and folic acid and regular monitoring for systemic vasculopathies.
Although NAION may present with findings similar to that of GCA, a classic presentation of NAION without GCA signs or symptoms may not warrant the usual GCA testing of a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). However, if there is any doubt then CBC, ESR, and CRP testing is indicated to rule out GCA. Patients should always be evaluated by a primary-care physician for potential modifiable or treatable risk factors including smoking, sleep apnea, hypertension, diabetes, hyperlipidemia, and other vascular disorders. Neuroimaging is only performed in cases diverging from a typical NAION course such as prolonged optic disc edema, progressing vision loss, or unusual pain. Except in cases of family history or personal clinical evidence, there is no proven value of additional vasculopathic or prothrombotic diagnostic testing (ex. carotid studies, hypercoagulability testing), however homocysteine levels may be tested in patients under the age of 50. Patients with significant hyperhomocysteinemia may be recommended supplementation of vitamins B6, B12, and folic acid and regular monitoring for systemic vasculopathies.
Differential diagnoses for NAION primarily include other anterior optic neuropathies or orbital lesions. Differentials include:
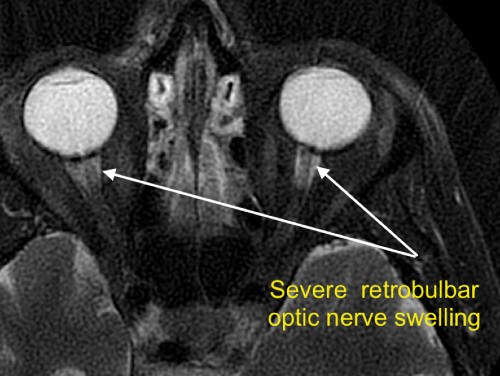
Optic neuritis may closely resemble NAION in regards to vision loss, visual field defects, optic disc appearance, and symptom onset; however key differences include age, pain with eye movement, and type of disc edema. Optic neuritis patients are generally younger, report pain with eye movement, and have diffuse disc edema without hemorrhages. Optic neuritis patients may also have retrobulbar optic nerve swelling in which case the optic nerve head appears normal. NAION disc edema is more likely to be altitudinal or segmental in nature and have disc pallor, vessel attenuation, and hemorrhages. Orbital lesions may result in compressive optic neuropathy and present as unilateral optic nerve head edema with slow, but progressive vision loss. However, orbital lesions also may cause lid proptosis, eye movement abnormalities, lid abnormalities, and non-resolving optic disc swelling. Infiltrative optic neuropathies, similarly, may demonstrate persistent optic disc edema and cause slowly progressing vision loss.
Many vasculopathies may trigger anterior or posterior ischemic optic neuropathy, the most common of which being giant-cell arteritis (GCA). Anterior ischemic optic neuropathy due to GCA is called arteritic anterior ischemic optic neuropathy (AAION). GCA has an annual incidence of 18 people per 100,000 in persons over the age of 50. Serious vision loss occurs in approximately 20% of these cases. The most frequent ocular manifestation of GCA is AION however both AION and PION may produce calamitous vision loss and therefore should be treated as an emergency. Although the clinical presentation of GCA and NAION are similar, systemic symptoms of GCA may be differentiating factors. Systemic symptoms of scalp tenderness, severe head pain, jaw pain, and general malaise oftentimes precede vision loss by weeks to months. Vision loss is also generally preceded by visual symptoms of transient blurriness or diplopia. However, known as occult GCA, one quarter of GCA patients present with isolated ischemic optic neuropathy and no systemic symptoms.
AAION induced vision loss is typically more serious than NAION with over half of AAION patients being unable to count fingers as compared to approximately a quarter of patients with NAION. AAION is considered an ocular emergency because untreated AAION involves the fellow eye in well over 50% of cases within days to week.
Optic nerve pallor is a differentiating factor between AAION and NAION as the affected optic nerve often presents immediately with pallor in AAION while pallor is delayed in NAION. While a “disc at risk” is suggestive of NAION, AAION may occur with any cup-to-disc ratio. Additionally, unlike NAION, GCA may also cause ischemia of the retina or choroid.
Erythrocyte sedimentation rate (ESR), C-reactive protein level (CRP), and complete blood count (CBC) should be performed on any patient over the age of 50 with ION who are being considered for GCA because contralateral vision loss is rapid and common. The results of the combination of these diagnostic tests is highly predictive for GCA (sensitivity of 97%). When these tests confirm GCA, the treatment generally entails high doses of intravenous steroids.
Various non-ophthalmic surgeries may cause severe bilateral vision loss by inducing anterior and posterior ION. Coronary artery bypass grafting and prolonged spinal-fusion surgery are the two surgeries most likely to provoke ION. However, it is worth noting that the reported incidence of this complication is less than 0.3%. For reasons that are unclear and likely multifactorial, cardiac surgery is more associated with AION while spinal surgery is more associated with PION. While the mechanism(s) are poorly understood, ultimately, axonal injury arises from either a vascular or compressive source.
Potential pathways for axonal damage include:
Proposed mechanisms contributing to these pathways include:
Risk factors for development of ION in patients undergoing spinal-fusion surgery in a prone position include:
Certain medications have been linked with NAION development to treat malignant tumors (ex. melanomas, leukemia, and lymphomas) and chronic hepatitis C, has been associated with bilateral, sequential NAION. The severity and prognosis vary, but some patients demonstrate recovery after discontinuing such medications. Potential mechanisms include systemic hypotension or deposition of immune complexes within the optic disc vasculature.
Three drugs prescribed to treat erectile dysfunction (ED) have been temporally associated with NAION onset, likely by producing systemic hypotension. Therapeutic doses of these ED medications may decrease systemic blood pressure over 10 mmHg. Each reported case connecting these medications with NAION occured in patients with “discs-at-risk”. The combination of these structurally crowded discs with augmented nocturnal hypotension is believed to have triggered an ischemic event. Despite the fact that the number of cases connecting NAION with ED drugs is modest, male NAION patients should be asked about ED medication usage. It is also pragmatic for patients being administered ED drugs to have a complete eye examination to assess for structural crowding of the optic discs.
Commonly used medicine to treat cardiac arrhythmias has been linked with an anterior optic neuropathy resembling NAION. It is worthwhile to mention that patients using this drugs generally already have vasculopathic risk factors predisposing them to NAION development. Several studies have revealed that NAION typically involves cases that are bilateral, have an insidious onset, involve general visual field loss (rather than altitudinal), and which have optic nerve edema persisting for months (rather than weeks).

NAION typically worsens over the course of two weeks before stabilizing, although several studies have demonstrated visual recovery of several lines of acuity in approximately 13-43% of cases. Once optic disc edema resolves, visual acuity generally does not deteriorate any more. The IONDT study, which observed patients 50 years of age and older, found that initial NAION visual acuities ranged from 20/20 to light perception only with approximately 50% of patients having a visual acuity of 20/64 or better and two-thirds of patients having a visual acuity of 20/200 or better.
Recurrence of an NAION event in an affected eye is rare, occurring in only 3-8% of patients. This is likely due to atrophy from the initial episode physically relieving crowding of the optic disc.

The IONDT study found that, within 5 years, roughly 15-24% of patients developed NAION in their other eye. Due to symmetry between the eyes, the fellow eye generally has similar vulnerability for an ischemic event due to similar structural crowding of the optic disc and systemic vasculopathies. Studies indicate that risk of fellow eye involvement is much higher in younger patients than older patients. One study found that the fellow eye was affected 35% of the time within only 7 months in younger patients.
Approximately 60% of NAION patients have at least one vascular condition. No large scale study has been performed to investigate an association between NAION and subsequent vascular events (ex. myocardial infarction or cerebral infarction). It is reasonable for physicians managing patients with NAION to consider the possibility of potential vasculopathies and to take proper precautions guided by evidence-based medicine.
It has been well established that antiplatelet medications, such as aspirin, are preventative for systemic ischemic events. The only antiplatelet agent examined for preventing NAION in the fellow eye is aspirin. The largest of these studies retrospectively examined 431 patients, of which 153 had received aspirin following initial NAION development.  At the 5 year mark, the probability of NAION development in the fellow eye was 17% in the aspirin group and 20% in the no aspirin group, with no significant difference between the two groups. Overall, studies investigating prophylactic aspirin use to prevent fellow eye involvement fail to demonstrate sufficient evidence to support aspirin therapy, but also demonstrate no increased risk of fellow eye involvement for aspirin users.
At the 5 year mark, the probability of NAION development in the fellow eye was 17% in the aspirin group and 20% in the no aspirin group, with no significant difference between the two groups. Overall, studies investigating prophylactic aspirin use to prevent fellow eye involvement fail to demonstrate sufficient evidence to support aspirin therapy, but also demonstrate no increased risk of fellow eye involvement for aspirin users.
Diabetes and sleep apnea are strongly associated with NAION with diabetes having been shown to be a risk factor for fellow eye involvement. Therefore, well-controlled diabetes and sleep apnea is imperative. However, one small study revealed 3 patients having developed NAION while being treated with continuous positive airway pressure (CPAP). %20management%20Ischemic%20Optic%20Neuropathy.jpg?width=597&name=continuous%20positive%20airway%20pressure%20(CPAP)%20management%20Ischemic%20Optic%20Neuropathy.jpg) Additional studies are needed to better understand the role of CPAP usage in preventing NAION for persons with sleep apnea. Other systemic conditions such as hypertension, hypercholesterolemia, and anemia have weaker associations with NAION. Given the vascular and ischemic nature of NAION, it is reasonable to assume that properly treating these conditions could potentially reduce the incidence of NAION as well as other vasculopathic conditions. One study suggested that NAION may be the initial manifestation of hypercholesterolemia in patients younger than 50.
Additional studies are needed to better understand the role of CPAP usage in preventing NAION for persons with sleep apnea. Other systemic conditions such as hypertension, hypercholesterolemia, and anemia have weaker associations with NAION. Given the vascular and ischemic nature of NAION, it is reasonable to assume that properly treating these conditions could potentially reduce the incidence of NAION as well as other vasculopathic conditions. One study suggested that NAION may be the initial manifestation of hypercholesterolemia in patients younger than 50.
Although smoking has not been found to be an independent risk factor for NAION, it is well known to cause poor cardiovascular health and therefore should be discouraged. Discontinuation of erectile dysfunction drugs is still disputed. ED medications produce systemic hypotension which potentially causes or contributes to NAION development. Studies indicate, but are inconclusive, regarding the role of nocturnal arterial hypotension in the development of NAION. Although NAION is found upon waking the majority of the time, this could be explained by approximately ⅓ of a person’s time being spent asleep and poor vision being more easily recognized immediately upon waking. Regardless, it may be prudent for antihypertensive medications to be taken in the morning rather than the evening to minimize the degree of systemic arterial hypotension.

