
Based on many conducted researches glaucoma is likely a PRIMARY VASCULAR DISEASE with initial damage to the optic nerve head and lamina cribrosa from blood supply deficiency. While intraocular pressure (IOP) is certainly a risk factor, glaucoma progression is likely more so related to ischemia from diminished ocular perfusion pressure (OPP) given that progression occurs with any IOP. Research outcomes from several decades provide strong evidence that glaucoma progression occurs from reduced ocular blood flow (OBF) specifically to the ONH when compensatory or alternative blood supplies cease to function. There is no doubt, that elevated or unstable IOP exacerbates and contributes to diminished ONH blood supply with subsequent ischemic injury creating a vicious cycle instigating further damage and progressive vision loss.

Historically, glaucoma was believed to occur due to elevated IOP especially as reduction of IOP is known to mitigate glaucoma progression. This raised IOP was assumed to inflict damage to the ONH via mechanical stress. Yet, this theory failed to explain why the vast majority of people with high IOP (i.e. ocular hypertension) never develop glaucoma and why many patients with normal or low IOP continue to experience vision loss due to glaucoma progression. In fact, research clearly demonstrates glaucoma can develop and progress with any IOP. These seemingly paradoxical data sets suggest an alternative mechanism of glaucoma, where damage is likely vascular rather mechanical in origin.
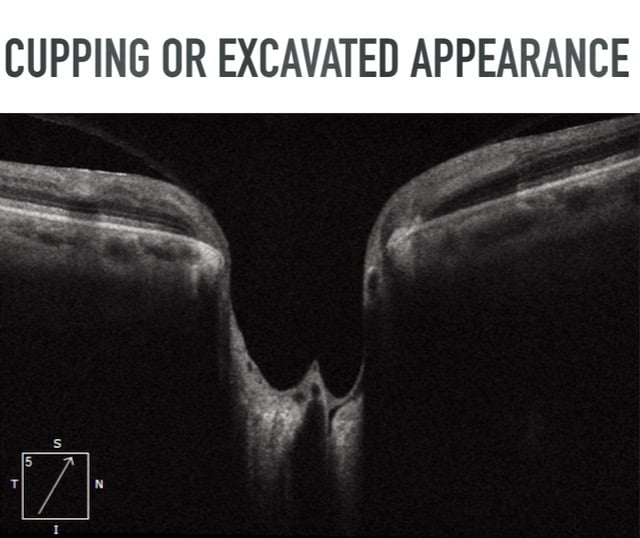
Stereoscopic ophthalmoscopy demonstrates an ONH with “cupping” or an “excavated appearance” from RGC axonal death near the peripapillary retina, disc, or anterior lamina cribrosa. This “cupping” or “excavated appearance” is an uncommon ONH finding considered highly pathognomonic for glaucoma. Clinical examination may reveal focal optic nerve rim thinning, vertically elongated cup-to-disc ratio, vessel bayoneting, peripapillary atrophy, or optic disc hemorrhages. Perimetry displays VF defects related to nerve fiber bundle damage such as: nasal step, arcuate scotoma, hemifield defect, or generalized defects commonly seen in advanced glaucoma.

Approximately 3-6 million Americans and 4-7% of people above the age of 40 years old have elevated IOP without evidence of glaucomatous optic nerve damage. Normal IOP ranges from 10-21 mmHg with a mean of 16 mmHg. Therefore an IOP of greater than 21 classifies an eye as being ocular hypertensive. This increased pressure may result from decreased aqueous drainage, increased aqueous production, or could be that eye’s normal, as IOP is measured on a bell curve. Patients with ocular hypertension (OHTN) do not experience any pressure sensation or blurred vision. OHTN is not accompanied by cupping of the optic disc, VF defects, thinning of the RNFL, or RGC loss, as this would denote glaucoma, not OHTN. Therefore, patients with high IOP in the absence of glaucomatous damage are referred to as having OHTN or being glaucoma suspects.
As no established standard of care existed for OHTN patients, the Ocular Hypertension Treatment Study (OHTS) was designed to evaluate the efficacy and benefits of initiating IOP lowering treatment to delay or prevent the onset of glaucoma. OHTS found that 5 years later the cumulative probability of glaucoma development for patients taking IOP lowering medication was only 4.4% and 9.5% in the untreated observation group. The OHTS results do not suggest that all patients with elevated IOP should be treated with ocular hypotensive medication and the researchers admit adverse effects of prolonged and indefinite medication use may exist, especially regarding financial and quality of life burden. Importantly, this study also identified risk factors for glaucoma, which were mentioned previously.

Notably, ONLY 9.5% of untreated OHTN patients developed glaucoma within 5 years. OHTS identified pertinent risk factors increasing the likelihood of OHTN patients eventually developing glaucoma. From the OHTS results, and similar studies, one can gather that ocular hypertension alone is not a sufficient or necessary factor for glaucoma development. Additionally, untreated OHTN patients have less than a 10% chance of developing glaucoma 5 years later. Said differently, over 90% of untreated OHTN patients will not proceed to develop glaucoma within 5 years. Such findings clearly demonstrate that while high IOP may raise the risk of glaucoma development and progression, high IOP alone does not warrant treatment with ocular hypotensive medication. Furthermore, 4.4% of the OHTN patients successfully treated with IOP lowering medication STILL developed glaucoma within 5 years. Moreover, the majority of major glaucoma studies (Advanced Glaucoma Intervention Study, Collaborative Normal Tension Glaucoma Study, Collaborative Initial Glaucoma Treatment Study, Early Manifest Glaucoma Trial) all demonstrate glaucoma progression despite significantly lowering IOP. These well-established outcomes indicate that glaucoma is far more complicated and multifaceted than elevated or fluctuating IOP alone.
Likewise, new research indicates there is no compelling evidence that postoperative transient IOP spikes in healthy eyes threaten optic nerve health and warrant treatment. The cessation of unnecessary IOP lowering treatments lessens clinician workload, decreases cost of medication for patients, reduces patient visits, and minimizes potential clinical and subclinical medication side effects.
While elevated IOP is an established risk factor for progression, perhaps a more significant risk factor is low ocular blood flow or ocular perfusion pressure (OPP). OPP is defined as the difference between arterial blood pressure and IOP. Therefore, both a high IOP and a low BP will lessen OPP potentially instigating ischemic damage to the retina and optic nerve. Research indicates that patients with low OPP have a considerably higher risk of glaucoma progression compared to patients with high OPP. Also, progression is associated with fluctuations in OPP from inconsistent BP or IOP. Nocturnal BP is normally lower due to diurnal patterns, however studies confirm progressive glaucomatous VF loss occurs in cases of exaggerated nocturnal BP drop.
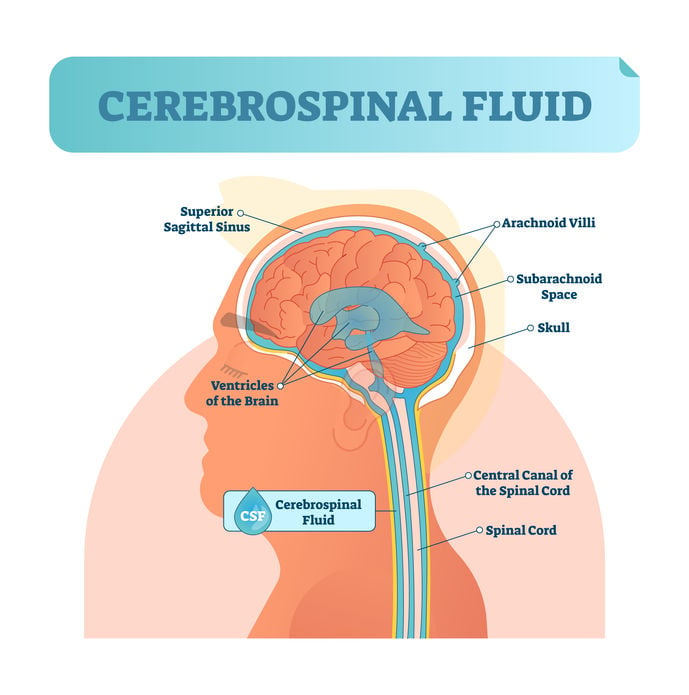
As research continues to support the concept of multiple pressure types having roles in GON, new findings suggest a previously overlooked intracranial pressure that may contribute to GON. Interestingly, initial studies in cats indicate an association between low cerebrospinal fluid (CSF) pressure and glaucoma development. Relatedly, human subjects with NTG have significantly lower CSF pressure compared to normal subjects. Similar research reveals that NTG subjects also have appreciably narrower orbital CSF space, which is associated with lower CSF pressure, when compared to high IOP glaucoma subjects. Given that glaucoma still develops and progresses despite normal IOP, it is plausible that NTG development and progression may partially arise from low orbital CSF pressure related to narrower orbital CSF space. Though research is ongoing, these initial results suggest that pressure behind the eyes can be as significant as pressure inside the eyes, especially in NTG patients.
.jpeg?width=500&name=Glaucoma%20Brain%20degeneration%20Restore%20Vision%20Clinic%20(1).jpeg)
As previously mentioned, though elevated IOP is certainly a risk factor for glaucoma progression, vision deterioration often still occurs despite successfully lowering IOP using medicinal and surgical treatments. Such instances suggest an IOP independent mechanism triggering this progression. Neuroimaging technology can potentially shed light on another side of glaucoma. For decades, glaucoma has been classified as a neurodegenerative disease by many researchers and clinicians. Similarities exist between neurodegenerative conditions, specifically Parkinson’s and Alzheimer’s diseases, and glaucoma regarding loss of neurons, transsynaptic degeneration, and cell death. Recent neuroimaging findings demonstrate that glaucoma patients have focal brain damage in other brain areas besides the retina and optic nerve. Brain tomography reveals structural changes of the lateral geniculate nucleus (LGN), optic radiations, and visual cortex associated with glaucoma.
Blog prepared in cooperation with Kaleb Abbott, O.D., M.S.
 Note: The information given in this blog are the opinions of the authors and for reader familiarization purposes only. This blog is not intended as a substitute for professional medical advice. Also, the information provided does not replace or abolish any official or legal terms for glaucoma diagnosis, treatment, and management. Authors are not liable for any undesirable consequences or effects related to the information provided in the blog.
Note: The information given in this blog are the opinions of the authors and for reader familiarization purposes only. This blog is not intended as a substitute for professional medical advice. Also, the information provided does not replace or abolish any official or legal terms for glaucoma diagnosis, treatment, and management. Authors are not liable for any undesirable consequences or effects related to the information provided in the blog.

