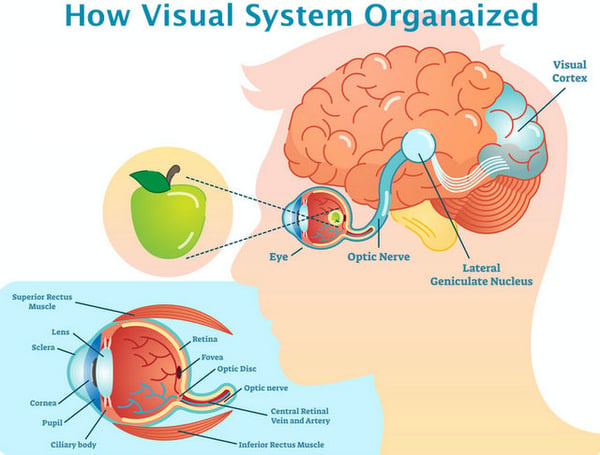
What is this nerve and why is it so essential to our sight? To answer this question we first have to understand what actually takes place in the physical act of seeing. Our visual system is comprised of three major parts: the eye, the visual cortex (located in the brain), and the pathway that connects them. 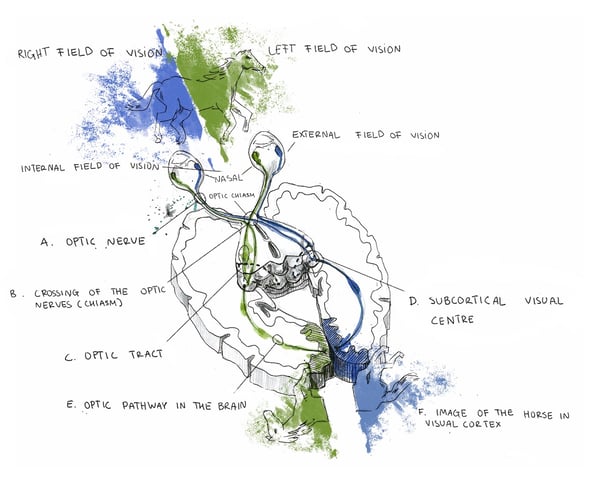 Within the eye is the retina, the cells of which are responsible for perceiving, processing, and relaying information to the brain, where the decoding of the received signals takes place and our actual visual experience occurs. The eye and brain are intricate, complexly structured organs, and their function in the visual process can’t be performed correctly if they’re not properly connected to each other. This is why the optic nerve, acting as a type of bridge between the two, plays such a critical role in how we see the world.
Within the eye is the retina, the cells of which are responsible for perceiving, processing, and relaying information to the brain, where the decoding of the received signals takes place and our actual visual experience occurs. The eye and brain are intricate, complexly structured organs, and their function in the visual process can’t be performed correctly if they’re not properly connected to each other. This is why the optic nerve, acting as a type of bridge between the two, plays such a critical role in how we see the world.
The optic nerve (occasionally referred to as cranial nerve II or CN II) is a structure consisting of millions of fibers and is responsible for everything from the dilation and contraction of the pupil (the light reflex) to how words and images are viewed up close or at a distance. Essentially, all visual signals are transmitted from the eye to the brain via this pathway, and as a result any injury to this nerve structure can cause vision loss, with the level of impairment depending on the severity and location of the damage. In turn, such damage can lead to drastic consequences for our lives and overall wellness.
Every day, thousands of people suffer from vision loss caused by optic nerve damage, and many individuals complain not only about their limited vision, but also limitations within the healthcare system itself. In fact, many visually impaired patients and their family members find that their healthcare providers do not treat their condition at all, or that the type of treatment offered doesn’t appropriately address their particular problem. These struggles—along with the difficulty of finding reliable information regarding various conditions and different treatments available—can cause considerable stress and doubt.
However, once a healthcare provider who attends to those with optic nerve damage is found, and relevant, practical information is obtained, patients can more accurately determine the most effective treatment method available, and whether or not their vision loss can be stabilized or partially reversed. This page is designed to provide such information and address the issues mentioned above, offering you an in-depth look at the optic nerve. It will guide you toward a greater understanding not only of what it is and how it works, but also what types of damage and disorders can occur and the various ways they can be treated.
The primary development of the human eye occurs between weeks three and 10 of the human gestational period. During the seventh week, the optic nerves—dual cylindrical structures that extend (one each) from the rear of the eyes—are derived from structures known as optic stalks in earlier stages of development. The evolution of the nerves continues through gestation and is sustained through the early years and into adolescence. During this term of development, very specific features and pathways are created which allow information received from the eye to pass successfully to the brain. An understanding of the structure, composition and visual pathway of the optic nerve (see figures above) is crucial for achieving a sense of its function and importance to the operation of sight.
STRUCTURE
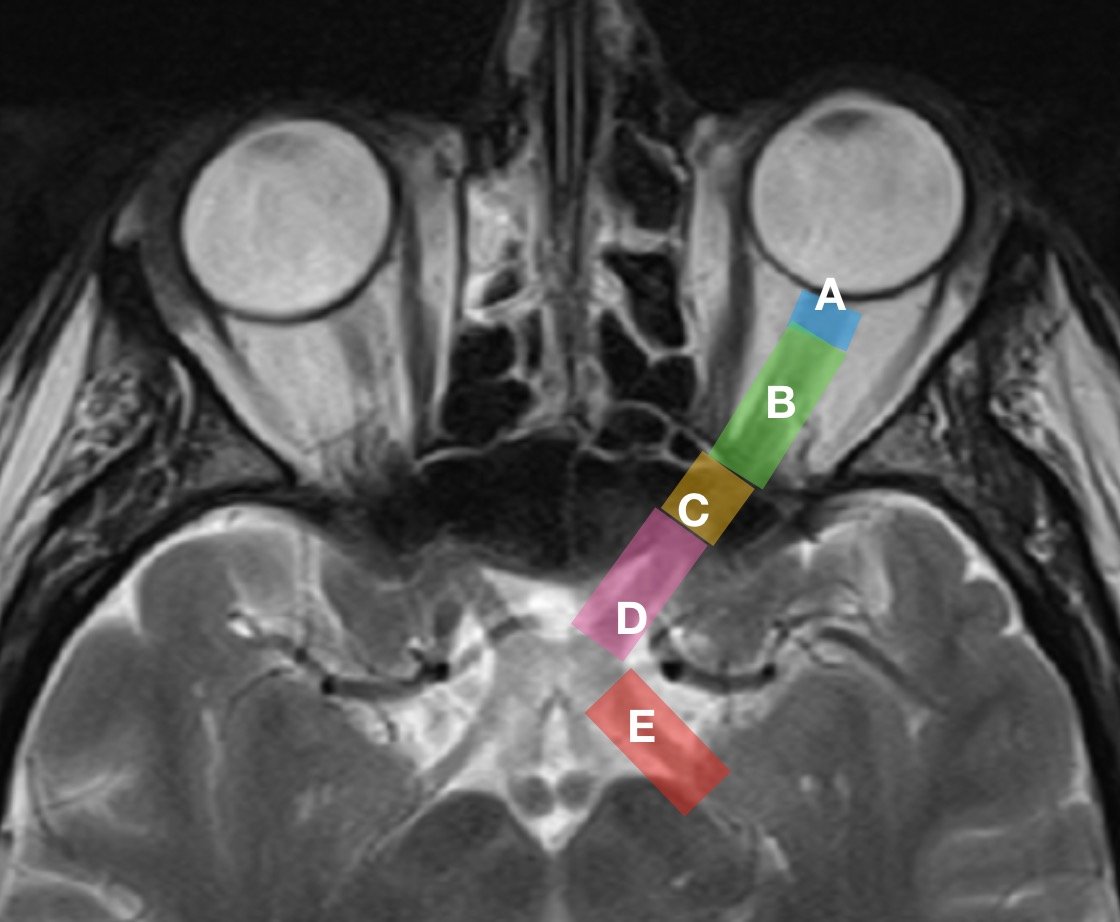
The optic nerve varies in length from person to person—and even differs between the two eyes of a single individual—but generally measures 35-55 mm. The most efficient way to describe the structure of the nerve is by dividing it into four main sections: (A) optic nerve head (or intraocular part), (B) intraorbital part, (C) intracanalicular part, and (D) intracranial part.
OPTIC NERVE HEAD (A)
The optic nerve head is a very unique part of the optic nerve as it marks a pivotal point of vascular, geometric and tonometric transformations. The optic nerve head—which may also be referred to as the optic disc or, more rarely, the “papilla”—is approximately 1mm in length and 1.5mm in diameter. The diameter and arrangement of the optic disc and the corresponding physiological cup depends upon the variable shape, size, and orientation of the opening into the Bruch’s membrane and the conically shaped chorioscleral canal.
The optic nerve head is a distinctive part of the nerve as a whole, and can itself be subdivided into three aspects: the surface nerve fiber layer, the prelaminar region and the lamina cribrosa region.
The surface nerve fiber layer—the most anterior (closest to the front) layer of the optic disc—incorporates the densely wound optic nerve fibers stemming from retinal ganglion cells across the whole retina as they merge and angle toward the optic nerve. This layer consists of a high volume of blood vessels, including sizable retinal vessels, venous channels and a tightly packed complex of capillaries.
The prelaminar region lies directly behind the surface nerve fiber layer, and is generally called the anterior part of the lamina cribrosa, although it can also be referred to as the glial or choroidal part. This region is one of the most essential areas of the optic nerve. It is composed primarily of glial tissue, a type of binding or connective tissue found throughout various parts of the nervous system. Glial fibers run perpendicularly to the nerve fiber masses and are significantly thinner than the coarser connective tissue fibers. This region also hosts a high number of capillaries surrounded by a membrane, which serve to aid and protect the nerve fibers as well as provide them with nourishment.
Where the prelaminar region of the optic nerve head is the anterior part of the lamina cribrosa, the lamina cribrosa region is known as the posterior part of the lamina cribrosa (or the scleral part).
The lamina cribrosa is a mesh-like structure composed of dense collections of collagen fibers as well as glial sheets. Similar to the prelaminar region, the nerve fiber groupings are protected by a glial membrane composed of glial tissue. The lamina cribrosa is central to regulating pressure levels between the interior of eye and the tissues that surround it.
INTRAORBITAL PART (B)
This part of the optic nerve, roughly 25mm in length, runs from the back of the eyeball to the opening of the optic canal. In this region, the optic nerve’s diameter is approximately twice that of the intraocular part, making it roughly 3-4mm wide. This is due to the myelination of the nerve fibers in this region and onward along the nerve’s length.
The myelin sheath is an extended and modified membrane wrapped around the optic nerve in a spiral fashion and aimed to be an electrical insulator. The function of myelin is to increase the speed of nerve conduction and neural circuits, and myelination serves as a source of plasticity in neural circuits.
This portion of the optic nerve is also surrounded by the meningeal sheath, which is made up of the arachnoid mater, pia mater and dura mater (the three meningeal layers), as well as cerebrospinal fluid. The dura mater and arachnoid mater are loosely joined near the back of the eyeball. Here there is greater subarachnoid space between the nerve and the sheath, creating a bulbous area behind the eye; the subarachnoid space between the nerve and the sheathnarrows as the nerve approaches the optic canal.
This part of the nerve contains roughly textured connective-tissue septa (septa being the plural of septum, a partition between chambers). These septa contain blood vessels, branch out in all directions, and are all connected to each other. It should also be noted that this part of the nerve rests in close proximity to the ophthalmic artery.
INTRACANALICULAR PART (C)
This part of the nerve lies within the bony optic canal and has a length ranging from 4-10mm. As with the intraorbital part, this portion of the nerve is also enclosed by the meningeal sheath. In fact, this part is virtually identical in its basic structure to the intraorbital section of the nerve discussed above.
INTRACRANIAL PART (D)
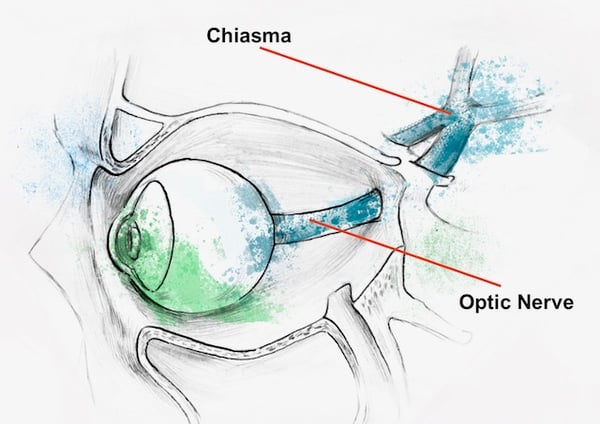
Finally, this section of the nerve, approximately 10mm long, extends from the rear opening of the optic canal, continues on above the diaphragma sellae and the cavernous sinus. At this point the optic nerve from one eye joins with that of the other eye, creating the optic chiasm.
OPTIC NERVE: ANTERIOR
The optic nerves are composed from axons (fibers) of retinal ganglion cells which gather together forming a trunk at the optic nerve, which then passes through the optic canal, within the cranial bones, and continues on to an intersection called the optic chiasm. The optic chiasm is a cross-like structure formed by the interweaving of nerve fibers. From this junction, the nerve fibers—now called “optic tracts”—extend to the lateral geniculate nucleus (or LGN) located in the thalamus. The whole of the thalamus is an essential relay center for sensory information received from various receptors, including the retina. It executes a primary analysis of incoming signals before their arrival at the occipital lobe of the brain, where the visual cortex is located. The LGN neuron’s fibers compose the next level of our visual pathway called optic radiation, which are responsible for conveying sensory information to the brain for further processing. Within the brain, the visual cortex then decodes signals from the retina and translates them into the real visual images we experience. This ultimately results in what we call vision.
OPTIC NERVE: POSTERIOR (E)
As you can see, even this general overview of the visual pathway can be somewhat difficult to understand. However, it can be simplified further by taking a closer look at the origins of this process: the cornea, lens, and particularly the retina and its cells.
The physical operation of sight is initiated when light reflected from objects passes through the cornea (the clear exterior part of the eye), and on through the lens. The lens’s primary purpose is to focus and direct that light onto the retina at the back of the eye, where chemical and electrical impulses (sensory information) are generated and passed on through the visual pathway to the brain. The retina’s connection to the optic nerve is essential to understanding the visual process and the nerve itself.
The retina is composed of several layers, including the layer of photoreceptor cells (two varieties: rods and cones), bipolar cells and retinal ganglion cells. Rods are responsible for processing black and white vision (including dim or low light), as well as our peripheral (or side) field of vision, which comes from signals captured by the rods. Cones are necessary for perceiving color and also play a role in our central vision, the type of vision being used while you read this text, for example. Before the information sent via the rods and cones can continue on its journey, it must be processed further by neurons, which produce high amplitude electric impulses (or “action potentials”).
These neurons are called Retinal Ganglion Cells, or RGCs, of which there are roughly one million in the retina. While these cells are variable in size and other physical and functional aspects, they share one key characteristic: each of them has a lengthy axon—a fibrous, thread-like part of a nerve cell—that physically extends and carries impulses all the way to the brain. RGCs are connected to corresponding neurons of the visual cortex, which, again, provides an analysis of the information obtained from the outside environment. In other words, the fibers from the RGCs are literally the building fibres of which the optic nerve is composed.
SUMMARY
Clearly, the optic nerve—its parts, composition and pathway—is amazingly intricate and highly complex. Its basic function, however, is relatively straightforward. It is an essential part of the central nervous system that serves to transmit it to the brain where that data is ultimately processed. In other words, structures— like our retina, optic nerve, higher visual pathways and subcortical visual centers—are essential and integral parts of a complex visual system in which data is gathered, transmitted and partially decoded. Keeping this core function in mind will help patients and information seekers better understand the centrality of the optic nerve to their overall health and wellness.

The most commonly known tumors are optic nerve gliomas, primary sheath meningioma, melanocytoma, malignant astrocytoma, astrocytic hamartoma, lymphoreticular tumors and metastatic tumors. Optic nerve tumors can be divided into primary tumors—which are tumors of the nerve—and tumors arising from the sheath. The most common tumor of the optic nerve is the optic nerve glioma, which are usually benign. However, some tumors such as gangliogliomas, medulloepitheliomas, haemangioblastomas and haemangiopericytomas are malignant gliomas. Meningioma is the most typical tumor of the optic nerve sheath. Primary sheath meningiomas arise from intraorbital or intracanalicular portions of the optic nerve. Secondary meningiomas are from intracranial sources. Most tumors cause gradual visual loss which progresses slowly and is clinically associated with further evidence of an anterior or posterior optic neuropathy, as well as compressive metastases and tuberculomas.

Glaucoma a leading cause of blindness—is a group of eye diseases that progressively and, in many cases, silently damages the optic nerve causing gradual and permanent vision loss. Generally, glaucoma is associated with increased fluid pressure within the eye, or intraocular pressure (IOP). At present, further damage to the optic nerve—or glaucomatous optic neuropathy—is avoided by lowering IOP, and the effectiveness of glaucoma treatment and management is measured by how well IOP is controlled. Reducing eye-fluid pressure in the eye through medications (eye drops) or surgery is a standard approach for treating glaucoma. But even with IOP lowered and stabilized, vision loss is not definitively prevented.

Depending on the segment of the optic nerve affected, ischemic optic neuropathies (IONs) are divided into anterior and posterior categories. Anterior IONs (AION) are subdivided into nonarteritic and arteritic etiologies. Arteritic anterior ischemic optic neuropathy (AAION) is caused by inflammation of arteries and requires immediate therapy to prevent blindness. The most common disorder associated with arteritic AION is giant cell arteritis (GCA). Non-arteritic ischemic optic neuropathy (NAION) is more common than arteritic AION, accounting for up to 95% of ischemic optic neuropathies. This condition is the result of the occlusion (or blockage) of small blood vessels supplying blood to the optic nerve head.
Traumatic optic neuropathy are subdivided into direct and indirect forms. Direct injury is the result of penetrating eye trauma, seen frequently with orbital fractures. Several varieties of direct optic nerve injury may be revealed as optic nerve avulsion, transection, optic nerve sheath haemorrhage, orbital haemorrhage and orbital emphysema. Avulsion usually follows severe orbital trauma with severe and immediate vision loss. Optic nerve transection occurs as the result of facial trauma or orbital fracture. Optic nerve sheath haemorrhaging causes potentially reversible visual loss, as opposed to the aforementioned conditions. Bleeding in the optic nerve sheath can be drained via a sheath fenestration leading to functional recovery (and an improvement in vision). Orbital haemorrhaging typically injures the optic nerve due to raised pressure within the orbit.

Hereditary optic neuropathies comprise a group of disorders which includes Leber Hereditary Optic Neuropathy (LHON) and Autosomal Dominant Optic Atrophy (DOA), also known as Kjer disease. Major lesions can be seen in papillomacular bundles which lead to the loss of central vision. This results in massive retinal ganglion cells (RGC) loss, seen clearly in the central region of the retina. More devastating, however, is that in most cases hereditary optic neuropathies are progressive. The pattern of transmission of the genetic deficit is employed for the classification of inherited optic neuropathies. They are autosomal dominant, autosomal recessive and mitochondrial. Often times, optic nerve dysfunction is simply a manifestation of more common diseases, which include various neurologic and systemic manifestations that cause multi-system degenerations.

Optic neuritis is an inflammatory condition affecting the optic nerve. It is idiopathic (or of an unknown cause) in most cases, but carries a strong association with multiple sclerosis (MS), where the demyelinating process is the main cause for developed optic nerve damage. In rare cases, other etiologies like infectious, inflammatory, and other pathological immunological responses play a role in this medical condition. Based on recommendations of North American Neuro-Ophthalmology Society (2012), optic neuritis is a clinical diagnosis related either to inflammatory demyelination of the axons connected with diagnosed multiple sclerosis (MS), or to idiopathic conditions, which typically occurred at age 20-50, of which approximately 75% are female.

Optic nerve hypoplasia (ONH) is characterised by an abnormally small optic nerve head frequently seen together with head cupping. Loss of vision occurs because the number of axons in the optic nerve are limited due to apoptosis during the development stages of the visual system. ONH is a unilateral or bilateral non-progressive underdevelopment of the optic nerve, and is considered to be a non-local syndrome rather than a more diffuse condition. It can be divided into three clinical subtypes: a) Optic Nerve Hypoplasia Simplex; b) Septo-optic dysplasia (de Morsier's syndrome); and c) Septo-Optic-Pituitary Dysplasia. Septo-optic dysplasia is considered to be a combination of ONH, pituitary gland hypoplasia and midline brain abnormalities.
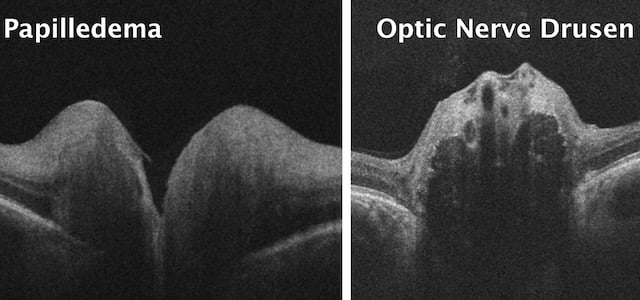
Optic Nerve Head Drusen (ONHD) is a relatively rare hereditary anomaly with structural abnormalities caused by white calcareous deposits in the pre-laminar region at the entire disc area. In most cases, they are generally asymptomatic and bilateral. ONHD are globular, calcified bodies accumulated within the optic nerve head. It is most commonly believed that the formation of disc drusen is caused by a chronic obstruction of axoplasmic flow, which leads to the formation of deposits. There is an agreement that ONHD is an autosomal genetic determinate abnormality and typically occur in small, crowded optic discs. Many disorders have been associated with optic disc drusen. However, it seems that the only true associations are with retinitis pigmentosa (RP). If calcareous deposits mechanically compress the axons of retinal ganglion cells, then this leads to resulting defects in the field of vision. Visual field defects can progress with age, and are often detected in the second decade of life. Although ONHD are typically benign, patients with diagnosed drusen should be monitored to rule out ocular complications that can be potentially sight threatening.

Radiation-induced peripheral neuropathy (RIPN) is a chronic handicap which is caused by compression of the nerve by fibrosis induced by radiation. In addition there may be evidence of direct injury to optic nerves through axonal damage and demyelination or injury to blood vessels by ischaemia. Radiation therapy for intra- and extracranial tumours can affect the anterior part of the optic nerve. Ophthalmological findings are those of acute ischaemic anterior optic neuropathy with acute loss in visual acuity. However, the damage to the posterior portion of the optic nerve or chiasma is the most frequent for radiation-induced optic neuropathy, with impairment of visual function.


Papillitis is an inflammation of the optic nerve head at its exit from the eyeball, or as "intraocular optic neuritis". The inflammation can lead to an acute loss of vision. The factors that cause papillitis include infectious diseases, disseminated inflammations, intoxications, allergic-hyperergic and immunological processes. Papillitis might have the same clinical signs as papilledema. However, papillitis may be unilateral, whereas papilledema is almost always bilateral.

Brain tumors can be malignant or benign. When benign or malignant tumors grow, they can elevate the pressure inside the skull and cause damage to brain tissue. Both benign or malignant tumours can damage the optic nerves, directly compress them, or damage them indirectly through increased pressure in the skull, ultimately causing problems with a patient’s vision. Generally brain tumors are categorized as primary or secondary. A primary brain tumor originates in the brain itself. Many primary brain tumors are benign. A secondary brain tumor, also known as a metastatic brain tumor, occurs when cancer cells spread to the brain from another organ, such as your lung or breast. Primary Brain Tumors can develop from brain cells, the membranes that surround your brain, called meninges, nerve cells or glands. In adults, the most common types of brain tumors are gliomas and meningiomas.

including single isolated optic neuritis (SION), relapsing isolated optic neuritis (RION), chronic relapsing inflammatory optic neuropathy (CRION), the neuromyelitis optica spectrum disorder (NMO), multiple sclerosis associated optic neuritis (MSON) and unclassified forms (UCON).
Cerebral vasular pathology is associated with diabetes, hypertension, and hypercholesterolaemia.
Traumatic brain injury (TBI) due to head trauma often leads to a broad range of visual impairments including double vision, photophobia and nystagmus. If the visual system at any level is damaged, more severe symptoms of TBI can be revealed, such as blurred and foggy vision, loss of field of vision and near complete vision loss. Damage to the optic nerve can occur due to both a penetrating injury and an indirect injury due to the transmission of traumatic forces to the optic nerve from a distance. There are two types of indirect traumatic optic neuropathy: anterior and posterior. The former can be caused by an avulsion injury due to the sudden rotation of the eye globe caused by blunt trauma. But most damages are indirect, with vision loss caused by a lack of blood supply through the central retinal artery.

- nutritional optic neuropathy, toxic amblyopia, tobacco, methyl alcohol.
- Tuberculosis, Syphilis, Lyme disease, meningitis. Viral infections (e.g., encephalitis, measles, mumps, rubella. chickenpox, herpes zoster, mononudeosis). Respiratory infections (e.g., mycoplasma pneumonia and other common upper respiratory tract infections)
Papilledema is a condition during which the axons of the optic nerve head are swollen and enlarged. This swelling is a reaction to elevated pressure in the cranium, and this condition can be a warning sign of a medical emergency that needs diagnostic and therapeutic interventions. It occurs most frequently in hydrocephalic patients. Other causes for papilledema are traumatic brain injury with a swollen brain, brain tumours, inflammation of the brain, haemorrhages, vascular events such as a lack of blood supply to the optic nerve (anterior ischemic optic neuropathy), or a blood clot due to very high ´blood pressure. In many cases papilledema is responsible for visual loss. Swollen axons undergo ischemia which causes damage, and finally it leads to developing defects (blind spots) in the field of vision.
Now, let’s discuss the most common symptoms typically related to optic nerve damage, divided here into four separate categories:
It should be noted that the symptoms explored here should be taken seriously, and if you are experiencing one or several of them, seek help from your eye care specialist as soon as possible.

Blurry vision, one of the most common visual symptoms reported by patients, refers to the loss or reduction of acuity, or sharpness. This causes objects in your visual field to appear out of focus. In the acute form, blurry vision affects one eye only. However, when the optic nerve or retina of both eyes is involved, blurriness becomes bilateral.  Blurry vision is often associated with refractive errors like myopia and hyperopia (nearsightedness and farsightedness, respectively) where objects may only appear blurry at a distance or up close. However, symptoms can also occur at all distances, as is the case with astigmatism. Blurred vision often causes one to squint in order to discern objects clearly, causing debilitating headaches and/or eyestrain. But blurry vision can be indicative of several different causes and ailments, and can be difficult to describe or may overlap or be confused with similar symptoms; eye care specialists will often have patients explain just what they mean by “blurry” during examinations. Blurry vision can be symptomatic of common and highly treatable conditions, but may also indicate the presence of more severe conditions as well, such as optic nerve or retinal structural abnormality. If your optician or optometrist cannot treat your blurry vision with corrective lenses, seek care immediately.
Blurry vision is often associated with refractive errors like myopia and hyperopia (nearsightedness and farsightedness, respectively) where objects may only appear blurry at a distance or up close. However, symptoms can also occur at all distances, as is the case with astigmatism. Blurred vision often causes one to squint in order to discern objects clearly, causing debilitating headaches and/or eyestrain. But blurry vision can be indicative of several different causes and ailments, and can be difficult to describe or may overlap or be confused with similar symptoms; eye care specialists will often have patients explain just what they mean by “blurry” during examinations. Blurry vision can be symptomatic of common and highly treatable conditions, but may also indicate the presence of more severe conditions as well, such as optic nerve or retinal structural abnormality. If your optician or optometrist cannot treat your blurry vision with corrective lenses, seek care immediately.
Much like blurry vision in its effects, hazy or foggy vision, often referred to and described as “cloudy vision”, refers to difficulties in clearly discerning objects due to a lack of contrast in one’s eyesight. Cloudy vision is often described as if one is looking through dirty or frosted glass.  Constant eye strain causes squinting, severe discomfort and headaches, just as with blurry vision. However, cloudy vision is different from blurry vision in that it seems as if one is peering through a thick haze or fog, or that one’s vision is “milky”, obscuring objects even further. Hazy or foggy vision can also be indicative of numerous acute or chronic conditions, both common and severe, such as glaucoma, cataracts, and acute optic nerve damage. It is one of the most typically reported symptoms among those suffering from problems with their eyesight, and can be distinguished during routine eye examinations.
Constant eye strain causes squinting, severe discomfort and headaches, just as with blurry vision. However, cloudy vision is different from blurry vision in that it seems as if one is peering through a thick haze or fog, or that one’s vision is “milky”, obscuring objects even further. Hazy or foggy vision can also be indicative of numerous acute or chronic conditions, both common and severe, such as glaucoma, cataracts, and acute optic nerve damage. It is one of the most typically reported symptoms among those suffering from problems with their eyesight, and can be distinguished during routine eye examinations.
Optic nerve damage often causes the loss of central vision which can be total (absolute) or partial (relative). In clinical practice this is defined as a scotoma (blank area in field of vision). %20Fedorov%20Restore%20Vision%20Clinic.jpg?width=600&name=Central%20scotoma%20(VF%20defect)%20Fedorov%20Restore%20Vision%20Clinic.jpg) Scotoma is caused by the damage of central fibers of the optic nerve, and frequently occurs in cases of optic neuritis and other autoimmune or inflammatory processes. Major complaints include severe difficulties with straight-ahead sight due to central vision being blurry, foggy, or entirely absent in the form of a blank area (as in the case of total scotoma). In the early stages of developed scotoma, another common complaint includes difficulties in distinguishing colors, especially between light or dark colors.
Scotoma is caused by the damage of central fibers of the optic nerve, and frequently occurs in cases of optic neuritis and other autoimmune or inflammatory processes. Major complaints include severe difficulties with straight-ahead sight due to central vision being blurry, foggy, or entirely absent in the form of a blank area (as in the case of total scotoma). In the early stages of developed scotoma, another common complaint includes difficulties in distinguishing colors, especially between light or dark colors.
Loss of Field of Vision/Low-Functioning Field of Vision: Most of the field of vision is included in the category of para-central or peripheral vision. A loss or lack of peripheral vision is often referred to as a “peripheral defect”, meaning that the typically wide field of vision has been reduced, leading to blank areas anywhere in the field of vision.  Most noticeable defects occur in the bottom of the field of vision, or the nasal or temporal parts. Depending on the severity of the case, patients describe their condition as partial loss, where the field of vision is not completely lost, but rather becomes low-functioning, with the individual experiencing hazy or blurry vision on the periphery. In severe cases peripheral vision is entirely absent. Extremely severe conditions such as advanced or terminal glaucoma leave only limited central vision preserved.
Most noticeable defects occur in the bottom of the field of vision, or the nasal or temporal parts. Depending on the severity of the case, patients describe their condition as partial loss, where the field of vision is not completely lost, but rather becomes low-functioning, with the individual experiencing hazy or blurry vision on the periphery. In severe cases peripheral vision is entirely absent. Extremely severe conditions such as advanced or terminal glaucoma leave only limited central vision preserved.  This is called “tunnel vision”, which means that central vision may remain intact and function normally, leading to the effect of seeing things through a tunnel or tube.
This is called “tunnel vision”, which means that central vision may remain intact and function normally, leading to the effect of seeing things through a tunnel or tube.
Loss of peripheral field of vision, and in many cases low-functioning field of vision, can make common activities like driving a car or walking difficult or impossible. Individuals suffering from loss or lack of field of vision often report difficulties seeing properly in low or dim light, as well.
Problems with field of vision often stem from different types of optic neuropathy or damage of visual system in the brain due to stroke or head trauma. Patients suffering from field of vision loss commonly seek the help of low vision specialists to determine ways that peripheral vision can be corrected or compensated by special lenses or devices or visual exercises. The cause and severity of the loss or lack of field of vision generally determines the effectiveness of various corrective treatments or rehabilitation approaches.
Glare: Glare is the difficulty in vision produced by bright lights when the luminance is much greater than the luminance to which the eyes are adapted.  Due to excessively bright light, poor visibility and poor visual performance is observed. In addition, recovery time from bright lights is longer than typically experienced. Glare is generally caused by an inability of photoreceptor cells in your retina to focus light received from your environment, and also depends on damaged retinal ganglion cells in the case of optic neuropathy. Glare is often described by patients as causing a “shimmer” or “halo” effect when trying to focus on a light-reflecting object or area in one’s field of vision. Like many other symptoms of neuropathy, this can cause one to squint while attempting to focus, causing painful eyestrain and headaches. Finally, glare can be caused by any condition affecting the retina and photoreceptor cells, and can be indicative of serious eye conditions.
Due to excessively bright light, poor visibility and poor visual performance is observed. In addition, recovery time from bright lights is longer than typically experienced. Glare is generally caused by an inability of photoreceptor cells in your retina to focus light received from your environment, and also depends on damaged retinal ganglion cells in the case of optic neuropathy. Glare is often described by patients as causing a “shimmer” or “halo” effect when trying to focus on a light-reflecting object or area in one’s field of vision. Like many other symptoms of neuropathy, this can cause one to squint while attempting to focus, causing painful eyestrain and headaches. Finally, glare can be caused by any condition affecting the retina and photoreceptor cells, and can be indicative of serious eye conditions.
Dimming of Vision: Dimming of vision refers to the effect of one’s sight becoming obscured, as if a light switch within the eye was being slowly lowered or a curtain was being drawn across an individual’s eyes.  Objects appear darker and less clear than they are in actuality, which can also make them appear blurry, hazy, or lacking proper contrast.
Objects appear darker and less clear than they are in actuality, which can also make them appear blurry, hazy, or lacking proper contrast.
This symptom is often caused by optic neuritis, or inflammation of the optic nerve and the fibers of which it is composed. The degree of dimming of an individual’s vision, in this case, depends on the severity of the inflammation of the nerve. Optic neuritis can be caused by a wide array of autoimmune conditions and inflammatory diseases. Any dimming of a person’s the eyesight can be a symptom of these and many other underlying illnesses, and should be examined immediately.
Slow Adaptation to Darkness: “Dark Adaptation” refers to the process of one’s eyes adjusting to a reduction in light occurring in a given environment. The ability to adapt to darkness is determined by the ability of photoreceptors (rods and cones) in the retina to respond properly to lower levels of light after having been previously exposed to brighter light. Therefore, any damage to the retina caused by illness or injury will affect an individual’s ability to adapt to light. In order to improve one’s level of dark adaptation, the underlying causes of the symptoms, which are significantly diverse, must be treated.

One of the most common complain, and perhaps the most important, is that of an overall reduction in confidence. Confidence levels affect every aspect of life, from mood to motivation to mental health. It can be difficult to gain and maintain confidence even with perfect vision, and, with vision impairment, it can be even more challenging. For that reason, returning patients to a confident state is one of the main priorities and aims of restoration therapy.
Outside of overall confidence, another exceptionally common effect of visual impairment reported by patients is problems with reading and sometimes a complete inability to read at all. We seldom realize how important the ability to read is in everyday life. Whether reading for pleasure, for work, or simply reading bills to be paid, this is a key skill and faculty for all of us in our own ways. When this ability is lost, it can have a markedly negative effect in several areas of our daily lives.

One more effect that patients report with great regularity is difficulty walking, particularly in a crowd. A reduced visual field (especially peripheral vision) can render the simple act of walking highly challenging and even dangerous. Many people report repeated incidents of bumping into walls, doorways, furniture, and other people. This can be embarrassing, but, most importantly, it can cause bodily harm and injury both to oneself and others. Trips, falls, and collisions have all been reported by patients who were simply walking, even very short distances. Once again, this can have a devastating effect on one’s confidence and self-esteem.

Aside from those mentioned above, by far the most commonly expressed effect of visual impairment is the inability to drive. Many of us are dependent on our cars and ability to drive in order to travel to and from work, run errands, arrive at appointments, see friends and family, and any number of other daily and weekly tasks. Even minor visual impairments can have a severe effect on one’s ability to drive properly and safely, ultimately endangering oneself and others.
In fact, the inability to drive is often connected to three of the other most common effects on patient’s lives: the inability to work, the urge to stay indoors, and everyday codependency. While these three effects can arise for different reasons, they are often connected to driving. Those dependent on their cars may no longer be able to travel to and from work, lose their willingness to leave their homes at all, and depend on others to drive them wherever they need to go. Each of these effects can significantly damage overall confidence and productivity.
 Note: The information given in this blog are the opinions of the authors and for reader familiarization purposes only. This blog is not intended as a substitute for professional medical advice. Also, the information provided does not replace or abolish any official or legal terms for glaucoma diagnosis, treatment, and management. Authors are not liable for any undesirable consequences or effects related to the information provided in the blog.
Note: The information given in this blog are the opinions of the authors and for reader familiarization purposes only. This blog is not intended as a substitute for professional medical advice. Also, the information provided does not replace or abolish any official or legal terms for glaucoma diagnosis, treatment, and management. Authors are not liable for any undesirable consequences or effects related to the information provided in the blog.
